
Using data to untangle the relationship between chronic pain and depression
People living with chronic pain are more likely to have treatment-resistant depression — or not receive any treatment at all. Dr. Jennifer S. De La Rosa hopes to address the unmet needs of this population.

Jennifer S. De La Rosa, PhD, is building a career around the unmet mental health needs of an often-overlooked population: people living with chronic pain. As a data scientist, she crunches the numbers to bring their hidden experiences into the open, where their unique needs can be better met. In so doing, she hopes everyone will reap the benefits.
After earning her doctorate in sociology from the University of Arizona, Dr. De La Rosa launched a career as a data scientist. In 2017, she came to the Department of Family and Community Medicine, where she is now an assistant research professor. She joined the U of A Comprehensive Center for Pain and Addiction as strategy director in 2021 — and found her niche, drawing from her background in sociology and statistics.
“The study of social inequalities easily encompasses the social reality of pain,” she said. “In fact, people who have social disadvantages are more likely to experience not only pain, but to experience life-limiting pain.”
While she primarily considers herself a pain researcher, Dr. De La Rosa has been especially interested in the neurological relationship between pain and depression.
“They run on the same highway, which is the nervous system,” she said. “There are specific parts of the brain that are activated in both chronic pain and depression.”
Building an evidence base
In just five years as a pain researcher, she has published a flurry of studies that paint a vivid picture of the emotional lives of people with chronic pain. One study found that nearly 1 in 20 U.S. adults experiences both chronic pain and depression or anxiety — and, as her team shared in a follow-up study, people with chronic pain are less likely to receive effective mental health treatment.
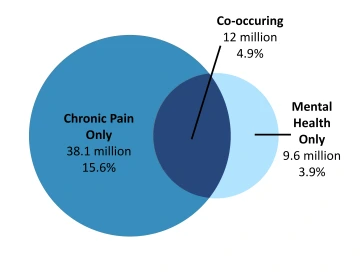
Dr. De La Rosa’s previous research found that around 12 million U.S. adults experience both chronic pain and untreated or treatment-resistant depression or anxiety.
“About 40% of people with chronic pain have a depressive disorder. Fully half of them are either not receiving treatment or they’re not receiving treatment that meets their needs,” Dr. De La Rosa said. “People with chronic pain are wildly overrepresented among people with unmet mental health needs.”
Her team’s newest study debunked a misconception that has been keeping people with chronic pain from participating in research. Anyone who has filled out paperwork in a doctor’s waiting room has likely encountered the Patient Health Questionnaire, which covers key depression symptoms.
“Somatic symptoms of depression are troubles with sleep, appetite, fatigue and slowing of movements — and many non-depressed people with pain have these symptoms,” Dr. De La Rosa said. “Could these screenings be inflating the rate of depression among those with chronic pain? We wanted to investigate.”
Mining an unusually robust dataset, Dr. De La Rosa and her team sought to improve on inconclusive studies by other groups.
“Our study was representative of the entire U.S. population and included the ability to compare those with and without chronic pain to those who are depressed and non-depressed,” Dr. De La Rosa said. “We found that lots of non-depressed people with chronic pain have somatic complaints, but they don’t translate into positive depression screenings. A positive screen is just as reliable in a patient with chronic pain as a patient without chronic pain.”
Opening the door to research
Scientists investigating new depression treatments strive to keep their data neat and tidy. They might see chronic pain as “noise” that distorts the relationship between depression and that new treatment.
“Right now, there’s a lot of interest in treatment-resistant depression, yet for the vast majority of studies, research is excluding folks with chronic pain,” Dr. De La Rosa said. “Our study shows there would be no scientific problem with including folks with chronic pain in depression research to develop treatments. In fact, this is the person who is most likely to show up in a clinic. Patients and taxpayers are interested in real-world validity.”
Dr. De La Rosa hopes the results of her latest study will lead to increased inclusivity in mental health research.
“People with chronic pain want to participate in studies. They can benefit just as much, if not more,” she said. “I see mental health and chronic pain groups joining forces to advocate for this kind of inclusivity — to develop treatments that could benefit everybody.”
Addressing stigma
Dr. De La Rosa feels immense satisfaction when she hears from patients who say her work makes them feel seen.
“That really makes me happy to know we are addressing a need — and one that has a lot of energy behind it once it’s tapped,” she said. “It’s exciting to see people get involved in advocacy or want to participate in research on the basis of our publications.”

Photo: Kris Hanning
Part of making people feel seen involves disentangling conditions like chronic pain and depression from the stigma that envelops them both.
“Stigma can increase the intensity of both depression and chronic pain. Social exclusion, rejection, being treated as untrustworthy — these experiences can increase the biological expression of pain and depression,” she said. “Many people with chronic pain have experienced someone suggesting their mental health is actually the source of their pain, and so maybe it’s not real. This is harmful and invalidating.”
Physicians can encourage patients to seek mental health support by validating their experiences.
“Patients will often need their stigma addressed to participate in care, feeling trust with providers. They need to be believed that their pain is real,” Dr. De La Rosa said. “Experiencing support instead of invalidation can quiet the central nervous system and have a therapeutic effect on the pain itself.”
Dr. De La Rosa believes cutting through this stigma is essential for physicians to support patients experiencing both chronic pain and depression.
“Pain can be quite depressing. Losing function, losing relationships, losing the ability to participate in your life, that’s about the most depressing thing I can imagine,” she said. “It takes guts to show up to life living with chronic pain and depression, so it is important that even the small steps people are taking are celebrated and encouraged.”